Introduction
Since the beginning of the COVID-19 pandemic, discussion around the repurposing of existing medications for use against SARS-CoV-2 has been a hot issue, and for good reason. When a novel virus emerges that both rapidly spreads and sends many patients to the hospital, we want to use every tool available to reduce morbidity, mortality, and transmission. This meant that from day one of the pandemic, physicians and scientists began scrambling to find tools and medications that could be used. The search began by looking for drugs used for previous coronavirus diseases such as severe acute respiratory syndrome (SARS) or Middle East respiratory syndrome (MERS), as well as in vitro experimentation.1 Some of the repurposed drugs that have been investigated include remdesivir, favipiravir, lopinavir-ritonavir, azithromycin, dexamethasone, hydroxychloroquine, and ivermectin.2
It wasn’t long after that these treatments became politicized among politicians, the media, and many citizens in the U.S. The malaria drug hydroxychloroquine was a major polarizing topic when it was promoted as effective by the Trump White House and subsequently criticized by their political rivals and the media. Nevertheless, it has been proposed that the FDA was pressured by the Trump White House to approve hydroxychloroquine despite incomplete evidence, contributing to quick approval for use under emergency use authorization (EUA).3 Soon after, the EUA was retracted by the FDA due to a lack of ability to replicate evidence for its use. Further research reviewed by regulatory panels suggests it was likely never effective in the first place, but this incident showed the power of political discourse around treatments.4
On one side, mostly conservative politicians and organizations are pushing for more widely available treatments. On the other side, mostly liberal politicians advocate the views expressed by the broader scientific, medical, and regulatory institutions, which are pushing for high-quality data to be available before treatments are used. This discourse has only continued with other repurposed drugs such as the anti-parasitic drug ivermectin, which has become a political hot topic to this day. The situation gets even more strange once we see the many organizations now passionately devoted to promoting the use of ivermectin for the prevention and treatment of COVID-19. They claim to present mountains of evidence suggesting ivermectin is safe and effective and could drastically reduce the morbidity and mortality of the COVID-19 pandemic. These groups claim to fight against censorship from regulatory agencies, social media companies, and big pharma who don’t want them to spread their message. Yet almost any professional scientific or medical organization makes a strong recommendation against the use of ivermectin for COVID-19. These panels of experts claim that there is a lack of sufficient safety and efficacy data to support its use, and that high-quality data suggests it is ineffective. Where is the disconnect between these two lines of thinking? How can we determine what is correct among multiple viewpoints with seemingly strong arguments?
The Argument for Ivermectin
The argument for ivermectin is well-summarized on multiple web pages which promote the use of repurposed medications, supplements, and at-home remedies. Some public domain web pages claim to accumulate all available data on ivermectin and compile it into a “meta-analysis”, or a summary of available research. They present colorful forest plots and a timeline of research. Interestingly, this webpage presents the same data summaries and plots for other repurposed treatments such as hydroxychloroquine, claiming high efficacy with “very high” confidence. Networks of many organizations have been formed which promote repurposed treatments, especially ivermectin. These include the Front Line Covid-19 Critical Care Alliance (FLCCC), Canadian Covid Care Alliance (CCCA), the British Ivermectin Recommendation Development Group (BIRD), and many more.5 Many of these groups were inspired by a senate hearing given by Dr. Pierre Kory, president and co-founder of the FLCCC, in December of 2020. In this hearing, he presented his evidence and spoke of ivermectin as “…essentially a ‘miracle drug’ for COVID-19”, and that it was profoundly efficacious in every stage of the disease.
Interest in ivermectin for COVID originates from June of 2020 when an Australian in vitro study analyzed the effect of ivermectin on SARS-CoV-2 infected cell culture. This resulted in a ~5,000-fold reduction in viral replication at 4 hours compared to control.6 This quickly caught the attention of many, who were initially very impressed and intrigued. Although many were quick to critique that the concentrations used in vitro were astronomically higher than could be achieved in plasma. The webpage c19ivermectin.com counters that with a 1990 article that found lung concentrations of ivermectin are much greater than plasma concentrations.7 Since then, many research studies have investigated possible mechanisms for this observation and experimented with the drug’s clinical use.11 Mechanisms of action theorized for ivermectin against COVID-19 include the blocking of nuclear import of viral proteins, inhibition of a protease needed for viral replication, competitive binding of viral S-protein, and anti-inflammatory effects.9 Computer modeling studies found ivermectin to have a very high binding affinity for SARS-CoV-2 spike protein.10 Other studies performed include mostly retrospective studies and small RCTs, many of which are pre-prints analyzing ivermectin and other repurposed drugs.11 These studies are all compiled and analyzed in an unpublished meta-analysis by ivmmeta.com, which found an 84% improvement for prophylactic use, 63% improvement for early use, and 40% improvement for late use after exclusion of what it deems to be low-quality data.
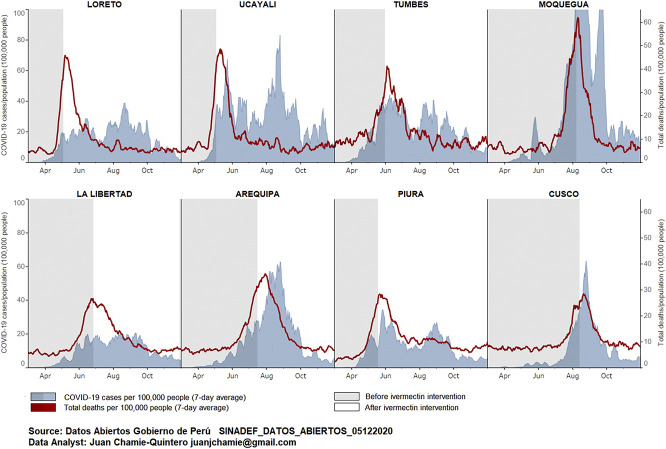
Proponents of ivermectin will often cite epidemiological data, which compare metrics of COVID-19 in large populations before and after their use of ivermectin. These are cases that purport to show decreases in COVID cases immediately following adoption of ivermectin treatment. Common examples cited are the widespread adoption of ivermectin for a time in Brazil, Peru, and Uttar Pradesh, India.12 Others include the relatively low case rates in African countries which had already distributed ivermectin as part of the African Program to Eliminate Onchocerciasis (APOC), which ran from 1995-2010 and distributed ivermectin once per year to eliminate this parasitic worm causing river blindness. These arguments are addressed in the next section.
Other organizations, such as the FLCCC, cite efficacy of “over 90%” for prevention of contracting COVID, and a 68-91% reduction in mortality with ivermectin, though there is no source cited for these numbers.13 They advocate for ivermectin, vitamin D, melatonin, other supplements and even mouthwash as a treatment protocol for COVID.14 The FLCCC announced last year that there is a “disinformation campaign” waged against ivermectin by public health agencies, including the WHO, FDA, and NIH. They argue that these organizations exclude key trial data from their analyses by maintaining a severely limited standard for acceptable data (large, well-designed RCTs, generally conducted on North American or European institutions). They term this as “Big RCT Fundamentalism” which neglects the data from smaller budget studies with lower-weighted evidence. In this announcement, the FLCCC calls for the immediate deployment of ivermectin globally to curb the pandemic. Additionally, they state that because Merck and Pfizer were investing in their own, novel oral antiviral medications that directly compete with ivermectin, they were incentivized to campaign against ivermectin, along with other “big pharma” companies.15
The Argument Against Ivermectin
Ivermectin is the latest of several repurposed drugs whose safety and efficacy have been clouded by widespread misinformation perpetrated on social media as well as by health and governmental authorities. Due to the initial promising in vitro results by Caly et al. and subsequent research suggesting the same, a flood of pre-prints and protocol records were disseminated across media platforms. Thus, the hype surrounding its use quickly rose and was even adopted by many clinicians, especially in Latin America.16 However, this excitement was entirely based on the premise these early promising results will carry forward to clinical settings, which there was far from sufficient evidence for. For example, even accumulated ivermectin concentration in the lungs is around 0.8µM, more than 50X less than 2.8µM, the half-maximal inhibitory concentration (IC50) found in vitro by Caly et al. in 2020.17 The original authors of the in vitro study have repeatedly stated that they do not think there is sufficient evidence to support the use of ivermectin in humans outside of clinical trials.18
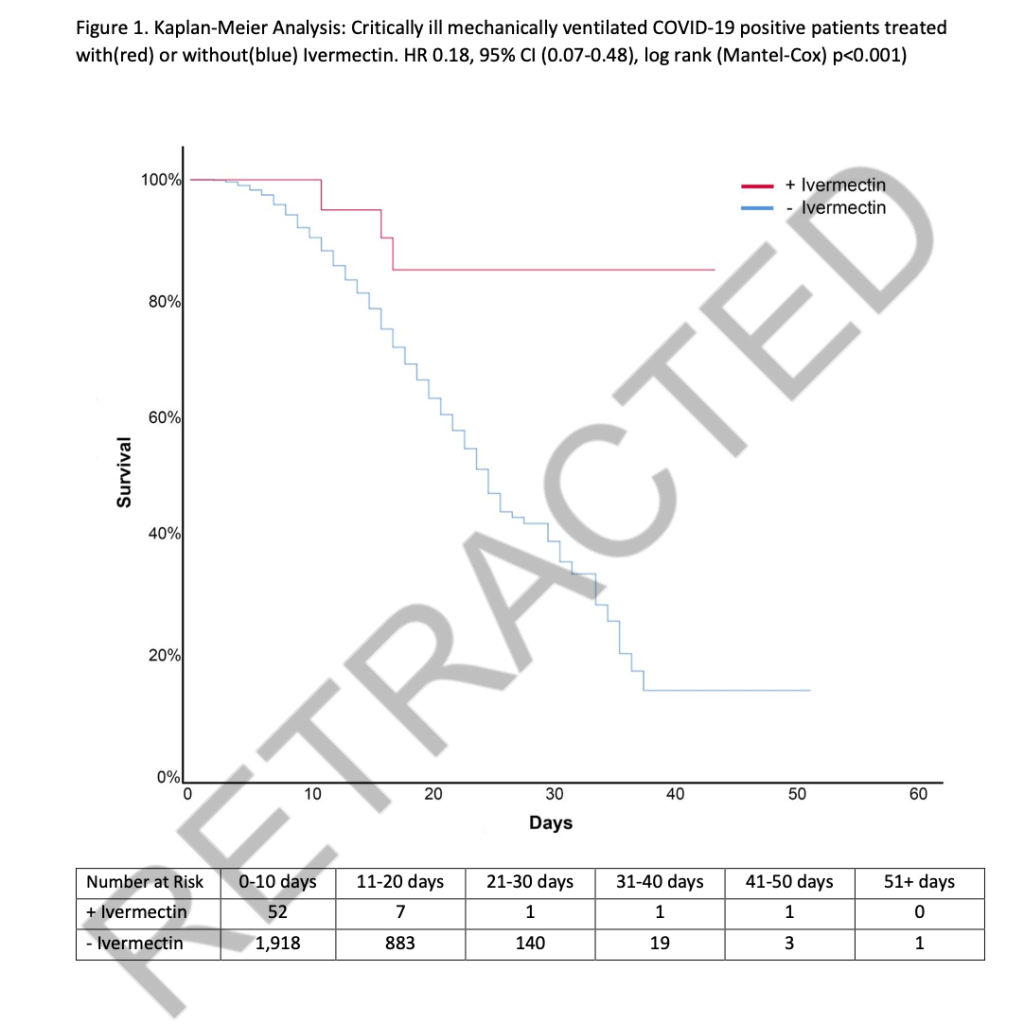
To this day, much of the original research on ivermectin have not made it past being pre-prints or protocol repositories. Several of the most notable early trials showing positive results were found to be using fraudulent data. The now retracted Surgisphere observational trial was a widely circulated pre-print used as the basis for several countries to adopt ivermectin use reporting 100% efficacy in reducing infection. However, after independent review the data were found to be likely fabricated.19 An array of other promising studies were also found to include fabricated data, improper randomization, or were never performed at all.20 Some peer-reviewed publications including RCTs are beginning to emerge. Yet many of these peer-reviewed papers are still methodologically limited by non-standardized dosing, heterogeneous populations, and uncontrolled interventions. Part of this can be explained by the difficulty of studying treatments in a rapidly ongoing pandemic, but this becomes a major issue when unreliable data are used as justification to use and push for widespread adoption of an unproven treatment. The abundance of rapidly circulating pre-prints and poorly designed trials make it extremely difficult for clinicians and patients to assess the landscape of available evidence.21 Meta-analyses by Kory et al. and others using these flawed studies are believed to have invalid conclusions because of the low quality of evidence compiled. Systemic fraud among ivermectin research was described in a letter to the editor of Nature Medicine, calling for better systems to detect fraud before use in meta-analysis.

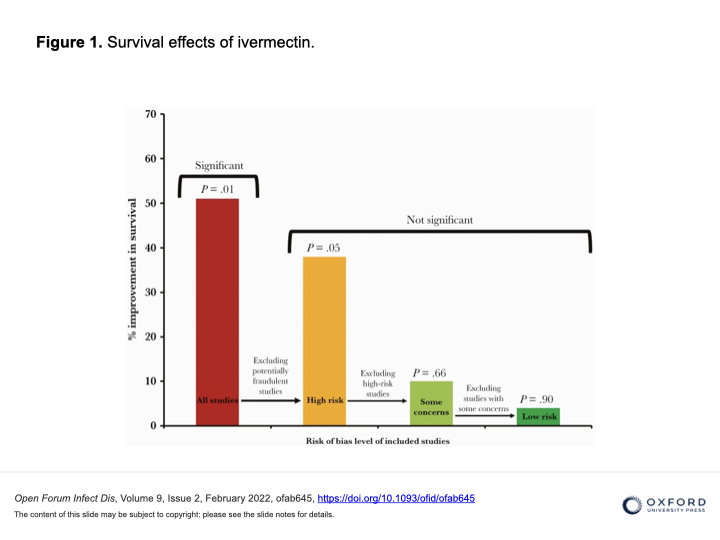
The unpublished meta-analyses found on ivmmeta.com among others do not follow any methodological or report guidelines, making their results unreliable at best. This “meta-analysis” does not use a standardized or recognizable method of statistical analysis, sometimes weighting small, non-randomized trials as heavily as large RCTs. Even still, the pooled estimates claimed to be presented on these websites have helped to cause a flurry of confusion and false confidence in ivermectin among clinicians, patients, and policymakers. Meta-analyses based on pre-prints and methodologically flawed trials result in unreliable data, as a meta-analysis is only as reliable as the data it analyzes.21,22 As they say: garbage in, garbage out. When the fraudulent studies are retracted and excluded from more recent reputable meta-analyses, the signal for benefit disappears.23
Thankfully, more recent research on ivermectin has lacked the methodological limitations of its predecessors. These have more accurately informed the scientific community about the efficacy of ivermectin. The TOGETHER RCT found no benefit to early treatment with ivermectin compared to placebo for risk of ER visits, hospitalization, or mortality. The I-TECH RCT found no difference between the ivermectin and standard of care arms in risk for progression to severe disease, and a non-statistically significant reduced risk of mortality for the ivermectin group. Both of these trials used higher doses than previous trials and recommended protocols, eliminating the argument that the dose was too low to see the effect.
These two randomized control trials (and the updated 2023 evidence listed at the end of this post) and multiple other well-designed studies are the primary data informing the current recommendation against the use of ivermectin for COVID-19 outside of clinical trials. Available evidence has been independently reviewed by panels in every major professional and regulatory organization, which have all come to this same conclusion. These panels consist of scientists and physicians who are experts at interpreting research in this field. Some notable panels which recommend against the use of ivermectin include the Infectious Disease Society of America (IDSA), the FDA, the WHO, the NIH, the CDC, the European Medicines Agency (EMA), and many other reputable, well-established professional organizations. A joint statement by the American Medical Association (AMA), American Pharmacists Association (APhA), and the American Society of Health-System Pharmacists (ASHP) strongly opposed the use of ivermectin to treat COVID-19 and called to an end of the use of ivermectin for COVID-19. Even Merck, the manufacturer of ivermectin, recommends against the use of ivermectin for COVID-19. The CDC issued an emergency press release to warn against inappropriate use of ivermectin for COVID-19, following a surge in poison control calls about ivermectin ingestion. This report urges healthcare workers to counsel patients against using ivermectin for COVID-19.
As experimental data surrounding COVID becomes less promising, many proponents of ivermectin have clung more and more tightly to epidemiological data. Common arguments include “what about Peru?”, “what about Brazil?”, or “what about Uttar Pradesh?” as strongholds that justify their faith in ivermectin despite scrutiny. No matter what kind of scrutiny individual trials get, the real-world, large-scale use of ivermectin in various countries showing declines in cases following use prove that there has to be something to ivermectin, right?

Unfortunately not. The ebb and flow of rising cases followed by declines happens in every country, whether using ivermectin or not. This happens as many factors combine, such as increases in community preventive measures and immunity from prior infection. These examples do not control for any of these confounding variables, and must be taken with a grain of salt. When the next wave comes, we see the same increases in regions using ivermectin as those not using ivermectin.
In Uttar Pradesh, all-cause mortality was anomalously low, where entire districts reported zero deaths from any cause for months at a time. This is likely due to the poor reporting infrastructure which was exacerbated during COVID. In fact, an analysis of public data under the right-to-information law estimates that the actual mortality in Uttar Pradesh was 43 times higher than officially reported. Uttar Pradesh is also a region that had some of the most extensive community interventions against COVID, such as strict lockdowns, a curfew, a mask mandate, and among the highest vaccination rates in India. These confounding variables make assessing the effect of ivermectin on a population level without control meaningless.
Some might make the point that if ivermectin is a relatively harmless drug that may or may not work against COVID, why not use it? The issue here is two-fold. First, ivermectin does have side effects such as dizziness, pruritis, nausea, and vomiting. Its use in an unregulated manner, in large doses, or from veterinary formulations has led to hospitalizations in multiple cases. It may also interact with other medications, such as blood thinners.24 Second, when a drug is hailed as the harmless magic cure for COVID being suppressed by those in power with an ulterior motive, it drives people to rely on ivermectin instead of other preventive measures. This can ultimately lead to more COVID deaths, dangerous drug interactions, confusion among patients and providers, and public division.
Another unfortunate but informative aspect is the behavior of some of the most proliferative groups and individuals promoting ivermectin. The right-wing network of healthcare providers called America’s Frontline Doctors (AFLDS) is a major promotor of ivermectin, as well as promotor of vaccine conspiracy theories. They offer telemedicine visits with doctors willing to prescribe ivermectin. However, patients are often left waiting on their medication for weeks or never receive them. AFLDS makes millions of dollars off these consultations. Simone Gold, ER doctor and founder of AFLDS was arrested by the FBI for rioting the capitol on January 6th. Dr. Pierre Kory, an intensivist and co-founder of the FLCCC lost or left three critical care jobs during the pandemic and now has his own practice where he treats COVID with his protocol for $400 and treats “post-vaccine syndrome” for $1250, which are likely not reimbursable by insurance. These ivermectin based treatments appear to be his only source of income. His co-founder, Dr. Paul Marik has been disciplined for prescribing opioids to people who are not his patients. He also claimed that Big-Pharma was suppressing his cure for sepsis that used vitamin C infusions. Marik has since had his clinical privileges suspended before resigning, and appears to no longer practice medicine. These cases do not inform of the efficacy of ivermectin, but we must take these potential biases, character traits and potential motivations into account.
How can we tell what is right?
If one thing is for sure, it is that the back and forth scrutiny of research regarding ivermectin is unusual. In many ways, it seems to be a battle between ideologies as much as it is a scientific debate. One side is fighting to utilize a widespread drug they believe has the power to stop the pandemic in its tracks. The other is fighting to ensure treatments are based on data-driven guidelines. One side fights against oppression by authority and corporations who do not have their best interest in mind. The other fights against the parallel infodemic of misinformation and disinformation perpetrated online. This distrust has led to efforts to influence clinical practice through lawsuits, ordering hospitals to use ivermectin for their loved ones against medical guidelines.25 Unauthorized prescription of ivermectin has soared, as have sales of veterinary formulations of ivermectin not intended for human use despite this being against regulatory guidelines and potentially dangerous.26 Over a matter of months, ivermectin went from an intriguing idea with promising signals to an almost cult-like belief and “vaccine alternative” for many. At first, the FLCCC described ivermectin as a bridge to the day that vaccines become available. As vaccines emerged, this nuanced language quickly disappeared while ivermectin is still touted as the magically efficacious prevention and cure for COVID. This has led the way for anti-vaccine activists to cling to the idea of ivermectin as the solution “they” don’t want you to know about, while fighting against “Big-Pharma’s profit-motivated vaccines”.
In conclusion
Ultimately, the preponderance of research with robust methods and reliable data suggests that ivermectin is not the miracle cure that it is made out to be. Rather than stoking more division with arguments based on ideology, we must use standardized methods of analysis to inform our decision-making. Otherwise, health policy will be up to whatever can garner the most hype and support. We should focus our efforts and discussion on the use of tools whose effectiveness is backed by high-quality, reliable research.
2023 Update
In addition to a Cochrane meta analysis published in late June of 2022, several large, well-designed RCTs have further suggested ivermectin has no beneficial effect on people with COVID-19. The most recent of which was published 2/2023 and investigates whether previous trials had been using too little ivermectin or were not treating patients for long enough to see the benefits. This trial found no effect from using ivermectin even at high dose for a long-period of time in ideal patients, and adds to the growing body of evidence suggesting ivermectin should not be used for COVID-19. A great resource for updated information is the JAMA “Ivermectin Resource Center”.
