A term that has rapidly gained traction since the 1990s is adrenal fatigue. Endocrinology societies say it is not a real medical condition, yet it continues to be commonly diagnosed and discussed by alternative medicine practitioners and naturopathic doctors. It is even more prevalent in the media and online where you may be led to believe your tiredness, irritability or palpitations are due to adrenal fatigue. Is adrenal fatigue based on real adrenal pathophysiology? Should providers be diagnosing and treating this condition? This post aims to provide a deep understanding of adrenal physiology and pathophysiology to answer these questions.
Adrenal Physiology
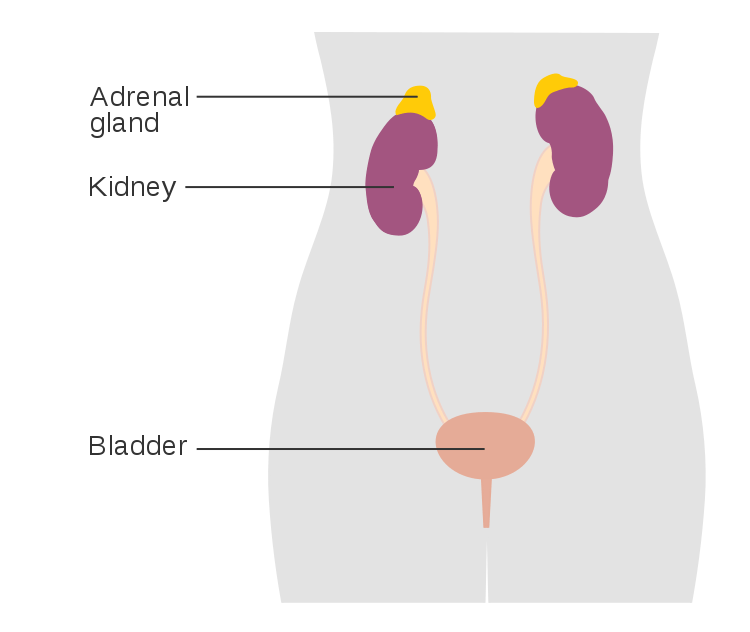
The adrenal glands are a set of extremely versatile and vitally essential endocrine glands located exactly where their name implies: above the kidneys. These bilateral pyramidal glands have many interconnected downstream effects. They are separated into layers based on the hormone secreted from the cells found there. The main regions are the outer cortex and an inner medulla which migrate together from separate cell populations around 28-30 days post-conception. The cortex is derived from cells called the mesoderm, while the medulla migrates into the cortex from cells called neural crest cells. All three layers of the cortex produce steroid hormones from the substrate pregnenolone, created from cholesterol. The medulla creates catecholamine hormones from dopamine.1
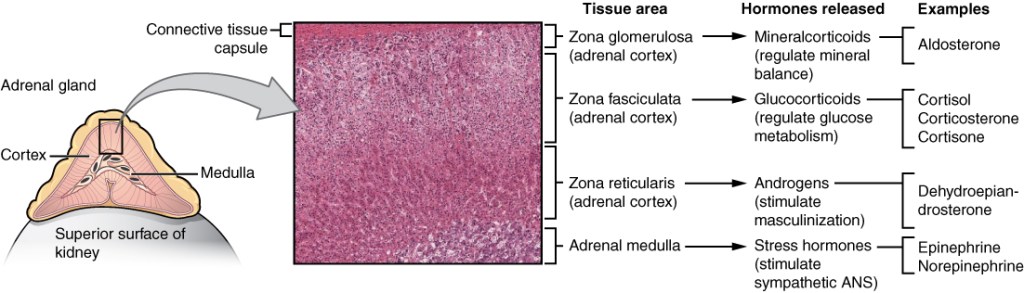
The outermost cortical layer is called the zona glomerulosa and produces a hormone called aldosterone. Aldosterone is a mineralocorticoid hormone that helps to regulate blood pressure by altering electrolyte and fluid homeostasis. This hormone binds steroid receptors in the renal nephron and distal colon to stimulate Na+ reabsorption and K+ excretion. This alters the osmolarity such that more fluid is retained and blood pressure is increased.2 This system is regulated separately from the other cortical layers, as it is regulated by the renin-angiotensin-aldosterone system (RAAS) and serum K+ levels. The RAAS is stimulated by decreased afferent arteriolar perfusion to the juxtaglomerular apparatus of the renal nephron. This stimulates the secretion of renin, which will cleave circulating angiotensinogen into angiotensin I. Angiotensin I will bind angiotensin-converting enzyme (ACE) receptors on the vascular endothelium of the lungs and kidneys, converting it into angiotensin II. Angiotensin II has many effects resulting in increased blood pressure, including the stimulation of aldosterone from the zona glomerulosa.3 Increases in serum K+ concentration will also up-regulate aldosterone synthesis, as K+ excretion is an effect of aldosterone.4
The middle cortical layer is called the zona fasciculata and produces an essential hormone called cortisol. Cortisol has many functions and is associated with a stress response. Cortisol will initiate mobilization of energy sources, enhancing hepatic gluconeogenesis and increasing blood sugar levels by reducing peripheral glucose uptake. Glycogenesis will also increase, ensuring an adequate supply of readily available glucose. Overall, cortisol is catabolic and will result in a reduced amino acid formation and reduced bone formation among other effects to ensure metabolic substrates are available for increased demands. It also reduces pain and is a strong immunosuppressive agent. In addition, cortisol is essential to regulating blood pressure as it will increase the sensitivity of vascular smooth muscle to catecholamines from the adrenal medulla.5 Cortisol is up-regulated by adrenocorticotropic hormone (ACTH), which is the communication molecule between the pituitary gland and the adrenal gland. It is part of the larger hypothalamic-pituitary axis or HPA. The HPA starts with a signal stimulating the up-regulated synthesis of hypothalamic corticotropin-releasing hormone (CRH), which increases pituitary ACTH secretion and goes on to stimulate the inner two layers of the adrenal cortex.6
The inner cortical layer is called the zona reticularis and produces the hormones dehydroepiandrosterone (DHEA) and androstenedione. These are precursor androgens, which will be converted to active androgens such as testosterone, dihydrotestosterone (DHT), or estrogen in the gonads, liver, adrenals, and peripheral tissues. In men, DHEA contributes a negligible amount to testosterone production as the testes make the vast majority of testosterone. The production of DHEA from the zona reticularis contributes to sex-specific features in both men and women. The zona reticularis, like the zona fasciculata, is stimulated by the action of ACTH on the cortex as part of the HPA axis.7
The adrenal medulla is the innermost zone of the adrenal glands and is home to the highest density of chromaffin cells in the body. Chromaffin cells are responsible for the production of catecholamines such as epinephrine and norepinephrine. These hormones will initiate the fight or flight response of the sympathetic nervous system, which includes contraction of vascular smooth muscle, enhancing cardiac contractility, pupillary dilation, piloerection, and relaxation of gastrointestinal smooth muscle. Epinephrine and norepinephrine will also induce metabolic changes that promote the availability of energy sources needed for fight or flight. These include increased glucagon secretion, decreased insulin secretion, and lipolysis. Catecholamine release is regulated by external stimuli which trigger catecholamine-filled vesicles by signaling nicotinic receptors located on the membrane of chromaffin cells. Further modulation of catecholamine release occurs by cortisol, which favors the conversion of epinephrine to norepinephrine.8
Adrenal Pathophysiology
Dysfunctions of adrenal gland function are complex and may result in either excess or insufficient production of adrenal products. They may be caused by dysfunction of any part of the HPA axis, including the hypothalamus, pituitary gland, or adrenals. They may be congenital or acquired. Diseases of excess or insufficiency may occur for any adrenal product, and we will cover a few of the most common. However, keep in mind that even the most common adrenal dysfunction is rare, with secondary adrenal insufficiency having a prevalence of 150-200 out of every 1 million people in developed countries.9
The most common adrenal dysfunction is adrenal insufficiency. This is a disease where the adrenals do not produce adequate cortisol or aldosterone, leading to fatigue, muscle weakness, weight loss, loss of appetite, and abdominal pain. If hypoaldosteronism is present, then hypotension or hyperkalemia may also manifest. It is most commonly caused by a loss of immune tolerance for cells in the zona fasciculata, leading to the autoimmune destruction of cortisol-producing cells – this is called Addison’s disease or primary adrenal insufficiency. Secondary adrenal insufficiency may be caused by an autoimmune reaction or tumor in the pituitary gland, resulting in insufficient levels of ACTH and therefore cortisol. Testing for adrenal insufficiency often involves an ACTH stimulation test, which may distinguish primary or secondary variants. The treatment for this condition is hormone replacement with a corticosteroid such as hydrocortisone for cortisol insufficiency, and a medication called fludrocortisone for aldosterone insufficiency.10
Another common adrenal dysfunction is Cushing’s syndrome. This is precisely the opposite of adrenal insufficiency, with excessive cortisol being produced from the adrenal gland. The most common cause of this is long-term, high-dose use of cortisol-like glucocorticoids used to treat other conditions. However, secondary Cushing’s syndrome may result from pituitary tumors causing excessive ACTH production – the most common endogenous cause of Cushing’s syndrome. Primary Cushing’s syndrome is caused by tumors of the zona fasciculata causing excessive cortisol secretion. High cortisol levels may result in weight gain, a round face, weak muscles, and wide purple abdominal stretch marks. Testing is complex but an initial diagnosis may be obtained from a 24-hour urinary free-cortisol test or a late-night salivary cortisol test. These aim to determine if your cortisol levels are chronically elevated and not following the typical 24-hour cycle. Surgical removal of the tumor responsible or modification of medications are the treatment for Cushing’s syndrome.11
Other less common adrenal disorders are briefly described here. An aldosterone-producing tumor of the zona glomerulosa may cause hyperaldosteronism, resulting in hypertension and hypokalemia. A tumor of the adrenal medulla called a pheochromocytoma may result in excessive catecholamines, resulting in hypertension, palpitations, headaches, or sweating. Congenital adrenal hyperplasia (CAH) is a group of conditions resulting in low cortisol production. This is most commonly from a deficiency in an enzyme used to make cortisol and aldosterone called 21-alpha-hydroxylase. The substrate of this enzyme builds up and is instead used to make androgens, resulting in a variety of reproductive disorders.12
Adrenal Fatigue
The term “adrenal fatigue” was coined in 1998 by James L. Wilson, DC, ND, Ph.D. who is a naturopath and an expert in alternative medicine “to identify below optimal adrenal function resulting from stress and distinguish it from Addison’s disease.”13 This condition is said to occur following prolonged stress which causes the adrenal glands to produce so much cortisol that they burn out and can “[no longer] adequately keep up with your level of stress”.14 Alternative medicine icon Dr. Mark Hyman, MD describes the origins of adrenal fatigue as “[the] chronic, unremitting, ongoing stresses of everyday life: stresses of our families, stresses of relationships, stresses of work, the stresses of constant interaction with Facebook and Twitter and the online world, and all these inputs that never let us pause.” Dr. Hyman goes on to say that if you have any of the following symptoms, you might just have adrenal fatigue: feeling tired and wired, irritability, trouble falling asleep, low blood pressure or low blood sugar, craving sweets or salts, or “just feeling kind of overwhelmed”.15
Symptoms like these plague many people, and it can be frustrating to have a doctor dismiss your symptoms as stress-related or even to have no answers at all. It must be a breath of fresh air to finally find a doctor who not only acknowledges your symptoms but seems to know the underlying cause of all of them – burned-out adrenal glands. The provider will likely even have supplements for sale that you can take to actively make up for your fatigued adrenal glands. The problem with this scenario is that this is more than likely false hope. The time spent testing for and focusing on a diagnosis like adrenal fatigue may be a distraction from serious underlying conditions. Many of the symptoms of adrenal fatigue are vague and common, but some may be signs of serious conditions. By focusing on adrenal fatigue, we may be overlooking real underlying conditions such as adrenal insufficiency, depression, chronic obstructive sleep apnea, or postural orthostatic tachycardia syndrome (POTS). Once a patient receives a diagnosis of adrenal fatigue, they may stop seeking a more accurate diagnosis.16 Additionally, there is currently not sufficient evidence that adrenal glands can burn out and stop producing sufficient hormones.17 In fact, the opposite is seen under chronic stress, which elevates cortisol levels.18 A 2016 review published in the journal BMC Endocrine Disorders found that there is no correlation between HPA axis function and the purported symptoms of adrenal fatigue. Additionally, studies claiming to support the validity of the diagnosis were found to have severe methodological issues and confounding variables.19
Adrenal Fatigue Treatment
One of the most glaring inconsistencies is that the vague and broad symptoms of adrenal fatigue only partly overlap with adrenal insufficiency, which is characterized by weight loss, joint pain, anorexia, nausea, vomiting, diarrhea, dry skin, hypotension, and fatigue.20 If a patient is diagnosed with adrenal fatigue, they are most likely not experiencing true adrenal insufficiency. However, they are often given ‘adrenal support’ supplements containing pregnenolone and other adrenal precursors which lead to excessive adrenal hormone secretion. Eventually, this may lead to desensitization of the adrenal glands and true adrenal insufficiency where the body can not properly respond to stressful events. This can last for months after discontinuing supplementation, and in extreme cases may lead to a life-threatening condition called adrenal crisis where the adrenals do not produce cortisol.21
These supplements are not regulated by the FDA, so their contents are not regulated. An analysis of adrenal support supplements found the thyroid hormone T3 in every supplement analyzed, and steroid hormones in most of them.22 These supplements are not inert and can have real and lasting effects on the people taking them. Supplements may even be made of ground-up bovine adrenal glands or hydrocortisone. The website of the originator of the term adrenal fatigue, Dr. Wilson, has an array of customized supplements called ‘Dr. Wilson’s Original Formulations’, with a price tag of $200 per 30-day supply of the ‘Adrenal Fatigue Protocol’ of 4 supplements.23 These are specially formulated by Dr. Wilson for stress-related adrenal fatigue, however, these products all come with the fine print stating that ‘This statement has not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.’. The lack of regulation for these hormonally active supplements with unknown ingredients or doses makes their use potentially harmful.24
Interestingly, many alternative practitioners diagnosing this condition may also recommend good lifestyle changes such as a whole-food, plant-based diet with high nutrient density, and avoiding foods that may contribute to inflammatory conditions. They may recommend stress management practices, consistent exercise, natural light, fresh air, good sleep hygiene, and more.25 These positive changes will likely make someone feel better even with other underlying conditions. However, they still may not address more serious underlying conditions contributing to their symptoms.
Adrenal Fatigue Testing
In some cases, practitioners diagnosing adrenal fatigue only use questionnaires or interviews to gather symptoms and form a diagnosis. However, lab tests analyzing the levels of various hormones are often used. The most common being cortisol, and a common brand being the DUTCH test, a $299 urine cortisol test measuring cortisol metabolites throughout the day to evaluate their 24-hour cortisol cycle.26 However, as the 2016 review mentioned earlier found, levels of cortisol metabolites are not correlated with fatigue symptoms and therefore cortisol testing is an inaccurate way to measure adrenal function. Additionally, the questionnaires used to evaluate adrenal fatigue symptoms are not scientifically validated and do not correlate with adrenal function.27 A separate systematic review of 108 studies found that post-traumatic stress disorder (PTSD) was not correlated with abnormal cortisol levels, despite being a condition of chronic stress.28 Worse still, the expensive adrenal fatigue tests are not covered by insurance, and therefore must be paid out of pocket by those taking them. In contrast, ACTH stimulation tests used to detect adrenal insufficiency are scientifically validated tests that provide actionable information about the function of the adrenal glands and the cause of the adrenal dysfunction.29 ACTH stimulation tests are inexpensive and often covered by insurance.
Addressing Adrenal Fatigue With Patients
As physicians, we may come across patients who have been told they have adrenal fatigue by an alternative practitioner and have been put on supplements, or they may have heard of the diagnosis and suspect they have it. If a patient comes to you that has been plagued by symptoms, the least helpful thing we can do is to disregard these as being all in their head or irrelevant. Their experience is real and might be seriously limiting their life experiences. We can acknowledge symptoms before agreeing on the etiology. First, we must listen to their experiences and validate them. Then we can state our opinion and if we think there are tests we can do to truly understand the cause of their symptoms. We might not know the answer to their problems right away, but we must assure them that we are doing everything we can to determine the cause of their symptoms by methods that are proven to be accurate.
In the meantime, patients might find benefit by following what has been described as the ‘adrenal fatigue diet’, which in reality is just a healthy dietary pattern. This diet consists of colorful, non-starchy vegetables, fruits, whole grains, healthy fats, and limited sodium consumption while avoiding refined fours, fried and fatty foods, alcohol, and caffeine.30 Other lifestyle habits such as getting good quality sleep, managing stress, and getting regular exercise may help them feel better. The main difference between the alternative approach and this one is that these changes are being implemented as a first step while we test to determine the underlying cause of the condition. These symptoms may be relieved by modifying lifestyle factors contributing to them, but we won’t be missing anything important while focusing on a narrow aspect of the endocrine system such as urine cortisol concentration.
Valid or Invalid Diagnosis?
Normal human physiology is extremely complicated, and as a result, human pathophysiology is an order of magnitude more complex. The pathological processes may be just as interconnected as the normal ones, which makes for difficult clinical problems for physicians to solve. When a patient presents with complaints ranging from fatigue, irritability, and difficulty sleeping or salt cravings, these may be manifestations of many completely unrelated processes; some important and others benign. However, it is important to account for the whole person and all of the factors that can contribute to their symptoms. When we take all of these symptoms and group them into a bucket under a vaguely defined and unsupported diagnosis we fail to fully address them. Adrenal fatigue can not be a valid diagnosis because the fundamental process described is inconsistent with known adrenal physiology and unsupported in the literature. The symptoms attributed to the condition are broad, vague, and unlikely to be related to adrenal function. The labs used to test for the condition do not provide clinically meaningful data, as they are not reflective of specific adrenal dysfunction. Finally, the supplements used are unregulated with hormonally active ingredients and are potentially harmful. Other treatments for adrenal fatigue are not based on clinical trials or expert consensus. None of the steps for the diagnosis of adrenal fatigue are based on expert consensus because the expert consensus is that adrenal fatigue is not a real disease. All of the major endocrinology societies have issued statements addressing adrenal fatigue as an invalid diagnosis.
On the other hand, conditions such as Addison’s Disease are valid diagnoses because there is a clear understanding of the pathophysiology and treatment. We understand the possible underlying pathophysiological mechanisms leading to dysfunction. More importantly, there are clear steps and guidelines on how to approach testing for the condition. After an initial cortisol measurement to identify abnormal values, further testing is performed to identify the location of the abnormality. An ACTH stimulation test checks to see if the adrenals are responsive to the signal or not. If the adrenals are normal, a CRH or insulin tolerance test checks to see if the issue is in the pituitary. Further narrowing down of the etiology of the condition can be performed with antibody tests and imaging to determine if it is from an autoimmune condition or tumor/calcification.31 Following standardized steps for evaluation of a condition ensures clinically meaningful data are collected and can be analyzed with standards that are based on well-supported guidelines.
Conclusion
Ironically, alternative practitioners aiming to provide holistic care may have focused so narrowly on cortisol levels and the adrenal fatigue hypothesis that they have failed to consider broader underlying conditions. This narrow view can lead to overlooking important underlying conditions that are contributing to their symptoms. In doing this, patients are being robbed of their ability to relieve their symptoms and are being led astray to a false diagnosis. In some cases, this may lead them away from addressing a life-threatening condition, and the treatments they are given may harm them. Nobody wants to be told that what they are experiencing is all in their head. To be given a tangible and logical-sounding diagnosis explaining all of their symptoms may help them feel heard and validated, and like they are finally addressing their condition. However, the actual cause of their symptoms may be thrown to the wayside while they are focused on treating a condition that almost certainly does not exist.

Thx Forrest. I am now prepared for patients that come in believing they have adrenal fatigue
LikeLiked by 1 person
Hi Sidney,
I’m glad you got something out of the article. Thanks for reading!
LikeLike
Very thorough! I appreciate the variety of topics that you take on.
LikeLike